国际肿瘤学杂志 ›› 2025, Vol. 52 ›› Issue (3): 144-151.doi: 10.3760/cma.j.cn371439-20241113-00022
来瑞鹤1, 滕月1, 戎剑2, 盛丹丹3, 耿羽智3, 陈建新2, 蒋冲4, 丁重阳5, 周正扬6( )
)
Lai Ruihe1, Teng Yue1, Rong Jian2, Sheng Dandan3, Geng Yuzhi3, Chen Jianxin2, Jiang Chong4, Ding Chongyang5, Zhou Zhengyang6()
摘要:
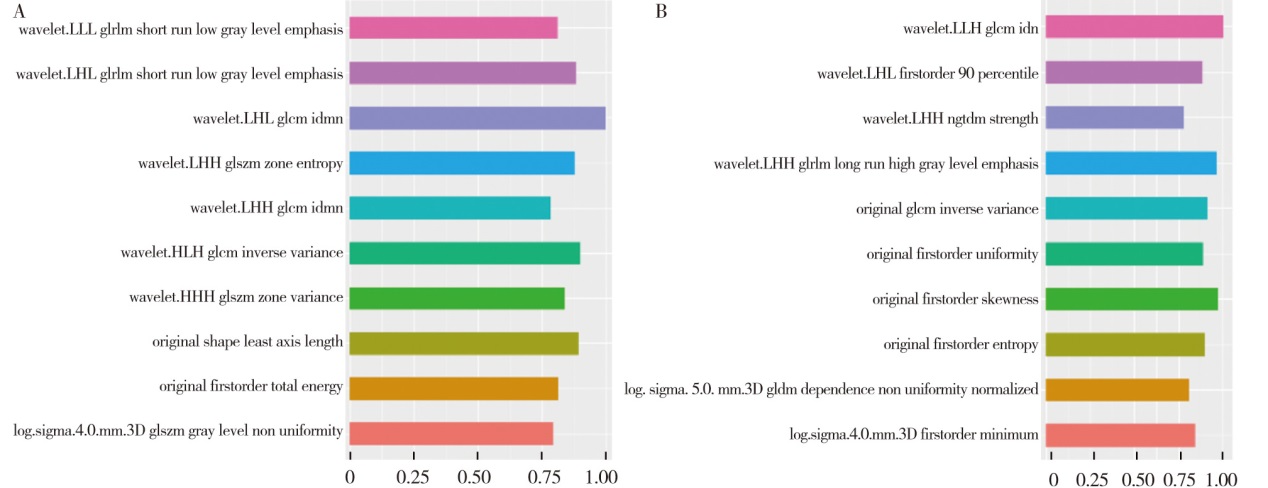
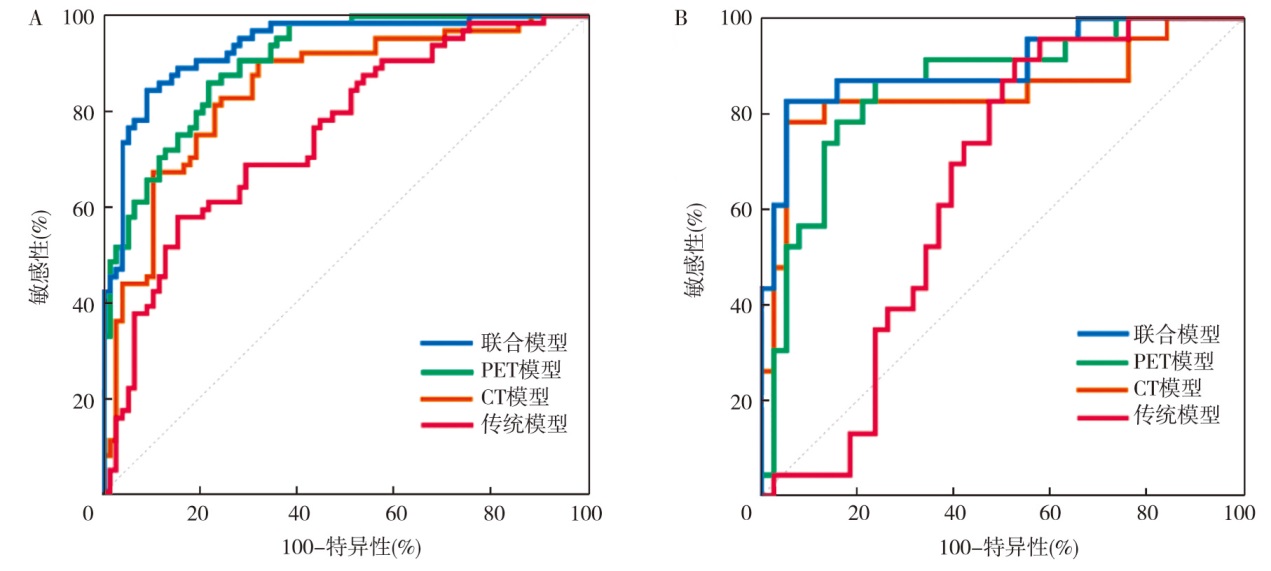
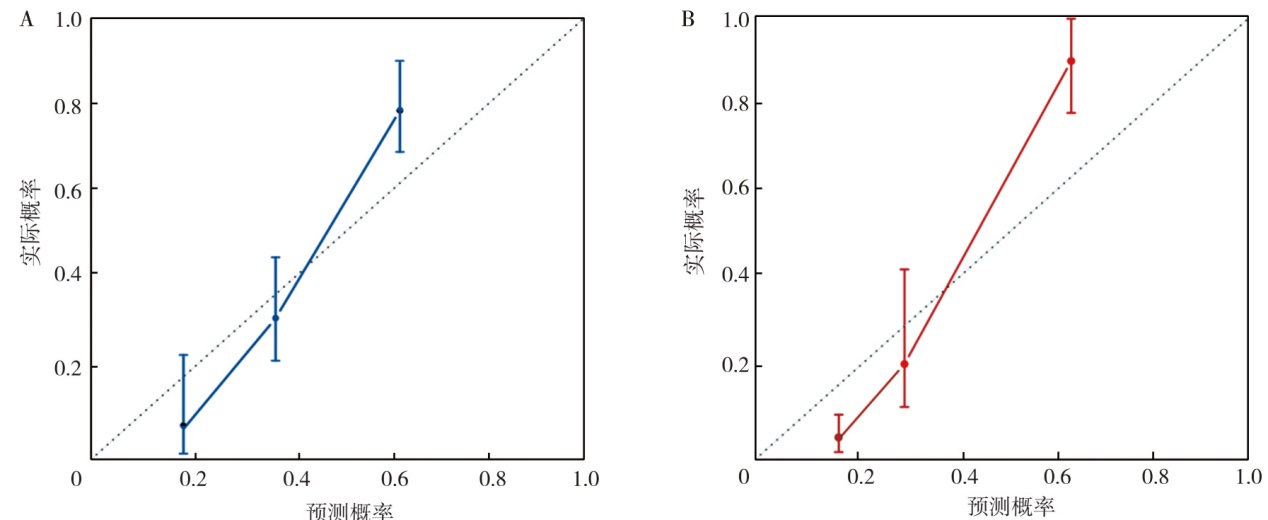
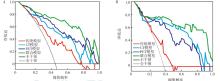
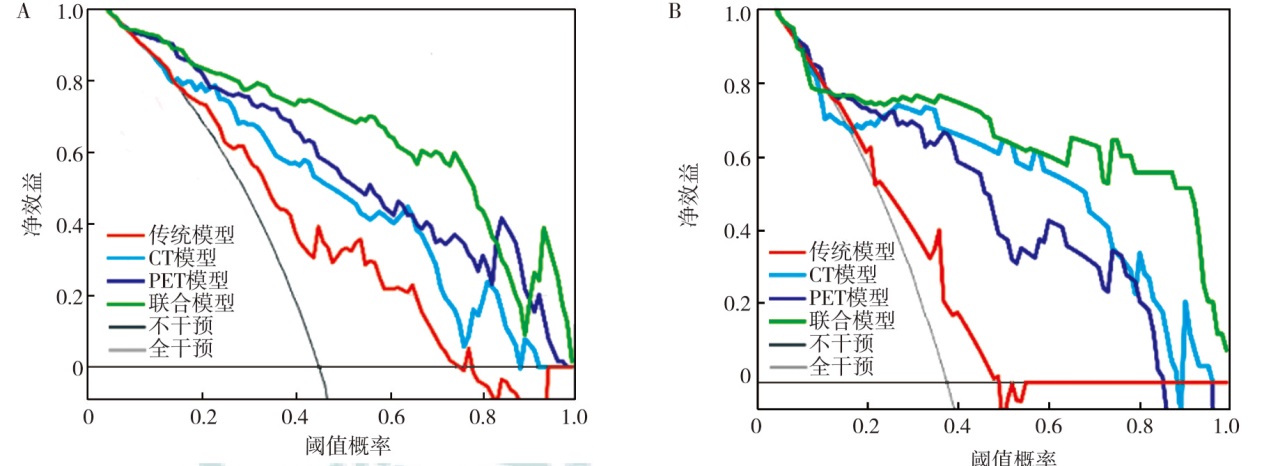
目的 评估基于原发灶18F-氟代脱氧葡萄糖(18F-FDG)PET/CT影像组学联合模型预测非小细胞肺癌(NSCLC)淋巴结转移的价值。方法 回顾性分析南京鼓楼医院2013年6月至2023年7月治疗前行PET/CT显像的203例NSCLC患者的临床资料。按照7∶3比例将患者随机分为训练集(n=142)和验证集(n=61)。在训练集中建立预测模型, 在训练集和验证集中分别对模型进行预测效能评估和临床应用价值验证。通过3D-slicer软件获得原发灶传统PET/CT参数和PET/CT影像组学特征。采用最小绝对收缩与选择算子(LASSO)、随机森林和极端梯度提升进行特征提取。采用支持向量机构建影像组学标签影像组学评分(Radscore)。采用单因素、多因素logistic回归分析预测NSCLC患者淋巴结转移的影响因素并建立模型, 采用受试者操作特征(ROC)曲线评估模型的预测效能, 采用校准曲线和临床决策曲线(DCA)评估模型的临床应用价值。结果 203例NSCLC患者中淋巴结转移116例, 其中训练集64例、验证集52例。采用3种互补的经典机器学习方法进行特征筛选, 最终分别得到10个影像组学特征。Radscore-PET的最佳阈值为0.43, Radscore-CT的最佳阈值为0.39。单因素分析显示, 性别(OR=0.48, 95%CI为0.24~0.95, P=0.036)、肿瘤标志物水平(OR=3.81, 95%CI为1.84~7.91, P<0.001)、肿瘤长径(OR=2.56, 95%CI为1.27~5.16, P=0.009)、肿瘤短径(OR=3.73, 95%CI为1.75~7.92, P=0.001)、空泡征(OR=0.32, 95%CI为0.12~0.86, P=0.024)、环形代谢(OR=3.67, 95%CI为1.33~10.13, P=0.012)、最大标准化摄取值(SUVmax)(OR=6.57, 95%CI为3.03~14.25, P<0.001)、肿瘤代谢体积(MTV)(OR=2.91, 95%CI为1.43~5.92, P=0.003)、病灶糖酵解总量(TLG)(OR=4.23, 95%CI为2.08~8.59, P<0.001)、Radscore-PET(OR=21.93, 95%CI为9.04~53.20, P<0.001)和Radscore-CT(OR=13.72, 95%CI为6.12~30.76, P<0.001)均是预测NSCLC患者淋巴结转移的影响因素。多因素分析显示, 肿瘤标志物水平(OR=2.55, 95%CI为1.11~5.90, P=0.028)、空泡征(OR=0.26, 95%CI为0.08~0.83, P=0.023)、SUVmax(OR=5.94, 95%CI为1.99~17.75, P=0.001)、Radscore-PET(OR=25.51, 95%CI为5.92~110.22, P<0.001)、Radscore-CT(OR=8.68, 95%CI为2.73~27.61, P<0.001)均是预测NSCLC患者淋巴结转移的独立影响因素。基于上述独立影响因素建立模型:传统模型(肿瘤标志物水平、空泡征、SUVmax)、PET模型(SUVmax、Radscore-PET)、CT模型(空泡征、Radscore-CT)和联合模型(肿瘤标志物水平、空泡征、SUVmax、Radscore-PET、Radscore-CT)。ROC曲线分析显示, 训练集中传统模型、PET模型、CT模型和联合模型的曲线下面积(AUC)分别为0.75(95%CI为0.67~0.82)、0.90(95%CI为0.84~0.95)、0.85(95%CI为0.78~0.90)和0.94(95%CI为0.88~0.97), 联合模型的预测价值高于传统模型(Z=5.01, P<0.001)、PET模型(Z=1.99, P=0.047)、CT模型(Z=3.25, P=0.001);验证集中传统模型、PET模型、CT模型和联合模型的AUC分别为0.65(95%CI为0.52~0.77)、0.86(95%CI为0.74~0.93)、0.85(95%CI为0.73~0.93)和0.90(95%CI为0.80~0.96), 联合模型的预测价值高于传统模型(Z=3.23, P=0.001)。训练集联合模型的敏感性和特异性分别为84.37%和91.03%, 验证集联合模型的敏感性和特异性分别为82.61%和94.74%。校准曲线显示, 训练集和验证集实际发生概率均与预测概率较为一致。DCA显示, 联合模型的辨别能力在训练集和验证集中均较好。结论 肿瘤标志物水平、空泡征、SUVmax、Radscore-PET、Radscore-CT均是预测NSCLC患者淋巴结转移的独立影响因素, 基于上述指标构建的联合模型对NSCLC淋巴结转移具有良好的预测效能和临床应用价值。