国际肿瘤学杂志 ›› 2025, Vol. 52 ›› Issue (3): 136-143.doi: 10.3760/cma.j.cn371439-20241021-00021
韩双( )
)
Han Shuang()
摘要:
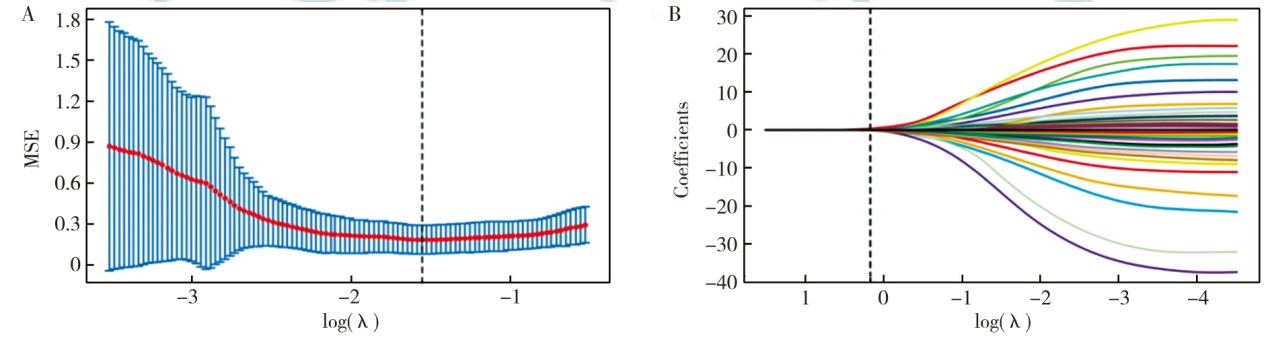
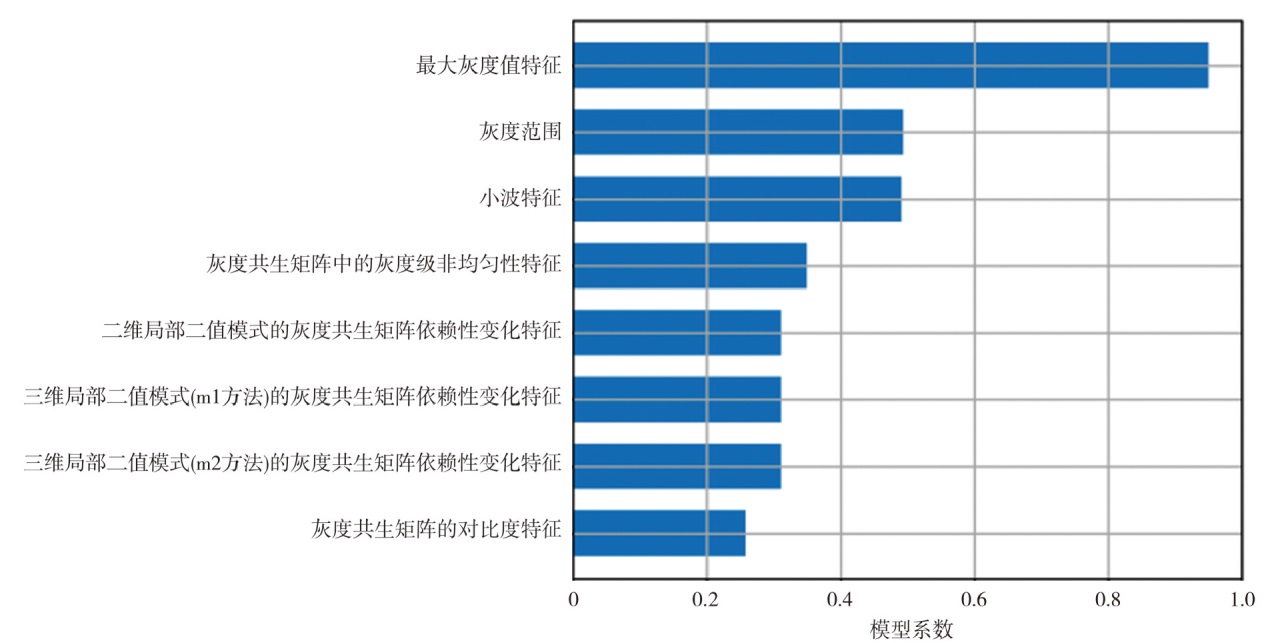
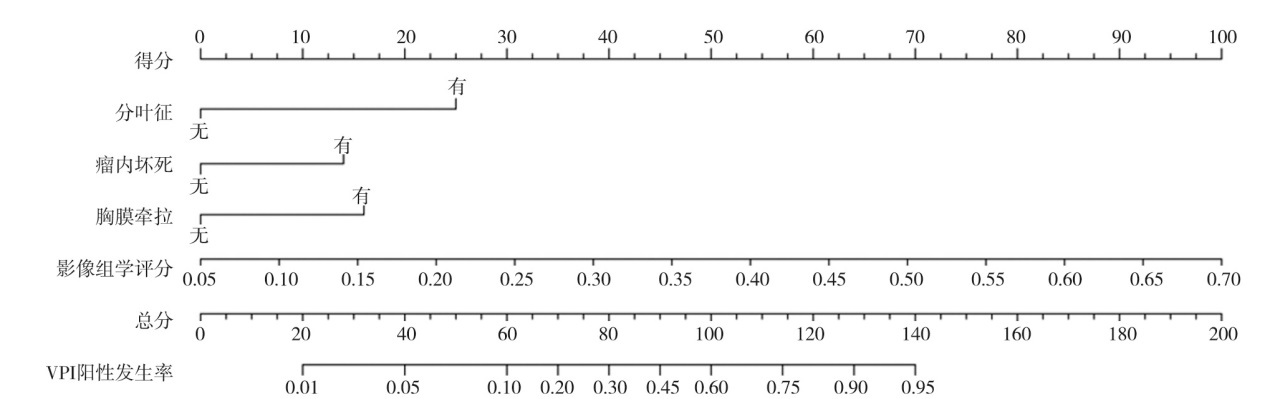
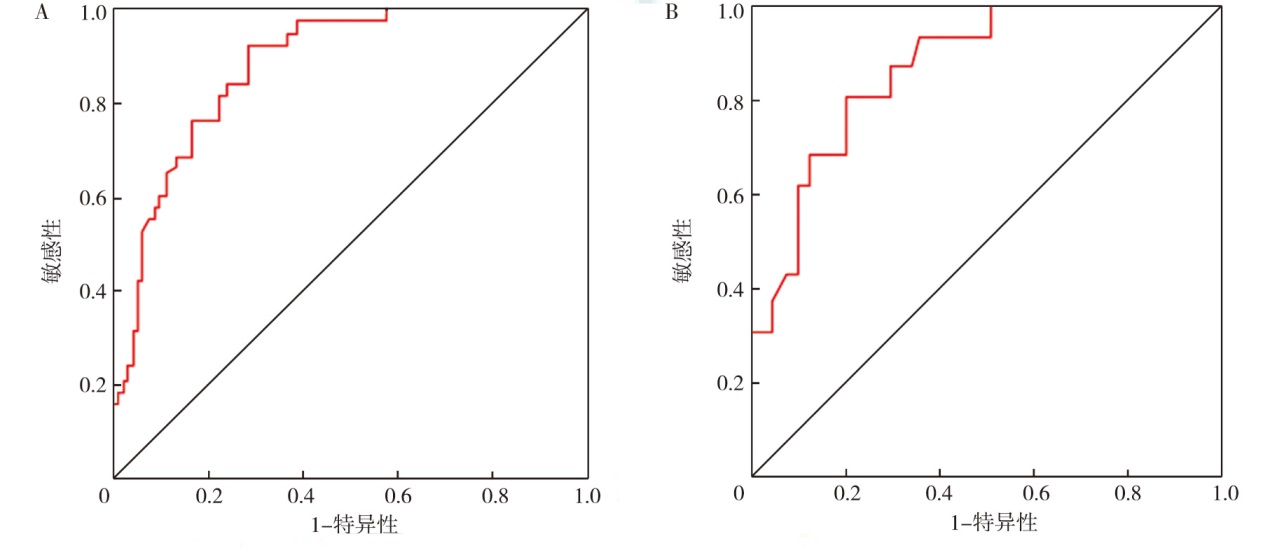
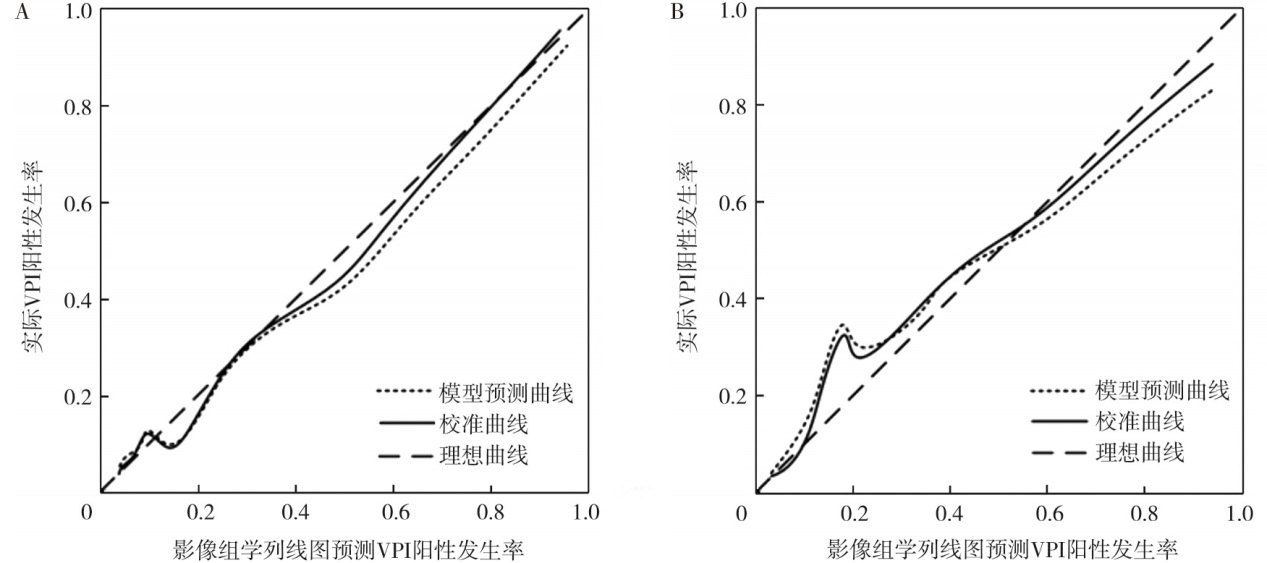
目的 探究外周实性结节Ⅰ期肺腺癌脏层胸膜侵犯(VPI)的CT特征及影像组学列线图的预测价值。方法 选择2022年8月至2023年11月贵州中医药大学第二附属医院收治的150例外周实性结节Ⅰ期肺腺癌患者为研究对象, 将2022年8月至2023年3月的患者定义为训练集(n=112), 2023年4月至11月的患者定义为验证集(n=38)。训练集用于建立模型, 训练集、验证集中分别进行模型性能评估。训练集中, 根据VPI发生情况, 将患者分为VPI阳性组(n=35)和VPI阴性组(n=77)。采用最小绝对收缩与选择算子(LASSO)回归分析对特征进行降维。采用多因素logistic回归分析预测VPI的影响因素, 根据多因素分析结果构建影像组学列线图预测模型。采用受试者操作特征(ROC)曲线及校准曲线评估预测模型的预测效能。结果 训练集VPI阴性组与阳性组患者的病理类型(χ2=11.49, P=0.003)、病灶最大径(t=5.83, P<0.001)、分叶征(χ2=9.29, P=0.002)、密度(χ2=8.32, P=0.004)、瘤内坏死(χ2=5.86, P=0.015)、胸膜牵拉(χ2=12.88, P<0.001)、胸膜接触(χ2=4.82, P=0.028)、邻近胸膜增厚(χ2=4.87, P=0.027)差异均有统计学意义。LASSO回归分析最终筛选出8个特征, 根据特征对应系数构建影像组学评分。单因素分析显示, 病灶最大径(OR=1.48, 95%CI为1.09~2.01, P=0.010)、分叶征(OR=5.09, 95%CI为2.31~6.00, P=0.001)、密度(OR=4.25, 95%CI为1.47~7.18, P=0.004)、瘤内坏死(OR=2.27, 95%CI为1.01~5.17, P=0.049)、胸膜牵拉(OR=6.75, 95%CI为1.92~13.68, P<0.001)、胸膜接触(OR=3.58, 95%CI为1.18~5.65, P=0.018)、邻近胸膜增厚(OR=3.60, 95%CI为1.18~5.72, P=0.018)、影像组学评分(OR=19 418.06, 95%CI为394.18~957 161.04, P<0.001)均是预测外周实性结节Ⅰ期肺腺癌患者VPI的影响因素。多因素分析显示, 分叶征(OR=6.42, 95%CI为1.42~18.58, P=0.018)、瘤内坏死(OR=3.63, 95%CI为1.01~10.01, P=0.046)、胸膜牵拉(OR=4.19, 95%CI为1.17~10.92, P=0.028)、影像组学评分(OR=179 711.20, 95%CI为525.13~61 552 573.59, P<0.001)均是预测外周实性结节Ⅰ期肺腺癌患者VPI的独立影响因素。将多因素分析中有统计学意义的指标建立影像组学列线图预测模型。ROC曲线分析显示, 训练集和验证集中, 影像组学列线图模型预测外周实性结节Ⅰ期肺腺癌患者VPI的曲线下面积(AUC)分别为0.88(95%CI为0.82~0.94)和0.87(95%CI为0.78~0.97), 敏感性分别为93%、82%, 特异性分别为72%、80%。训练集和验证集的C-index分别为0.89(95%CI为0.84~0.96)和0.88(95%CI为0.78~0.99), 两集的校准曲线均与理想曲线拟合良好。结论 外周实性结节Ⅰ期肺腺癌VPI的CT特征为有分叶征、瘤内坏死、胸膜牵拉, 基于CT特征的分叶征、瘤内坏死、胸膜牵拉、影像组学评分构建的影像组学列线图预测模型对外周实性结节Ⅰ期肺腺癌患者VPI具有较高的预测效能。